752
Views & Citations10
Likes & Shares
Gender Based Violence (GBV) is any act ‘that results in, or is likely to
result in, physical, sexual or psychological harm or suffering’ that is
directed against a person because of their biological sex, gender identity or
perceived adherence to socially defined norms of masculinity and femininity.
GBV includes intimate partner violence and can be physical, sexual, emotional,
economic or structural where that violence targets someone because of their
gender or non-compliance with gender norms. The aim of the guidelines is to
provide an adequate and integrated intervention in the treatment of the
physical and psychological consequences that in particular male violence produces
on women's health.
Keywords: Gender based
violence, Woman health
INTRODUCTION
Gender Based Violence (GBV)
is any act ‘that results in or is likely to result in, physical, sexual or
psychological harm or suffering’ that is directed against a person because of
their biological sex, gender identity or perceived adherence to socially
defined norms of masculinity and femininity. GBV includes intimate partner
violence and can be physical, sexual, emotional, economic or structural where
that violence targets someone because of their gender or non-compliance with gender
norms. It can be experienced by women and girls, men and boys, and transgender
and intersex people of all ages and has direct consequences on health, social,
financial and other aspects of their lives [1].
GBV takes on many forms and
can occur throughout the lifecycle, from the prenatal phase through childhood
and adolescence, the reproductive years and old age [2].
Types of GBV
The WHO divided GBV in two
groups:
·
Gender-based violence:
o
Rape by strangers
o
Female genital mutilation
o
Sexual harassment in the workplace
o
Selective malnutrition of girls
·
Domestic/Family violence:
o
Child abuse
o
Elder abuse
Intimate partner violence
and sexual abuse of women and girls in the family are overlapped in these two
groups [3].
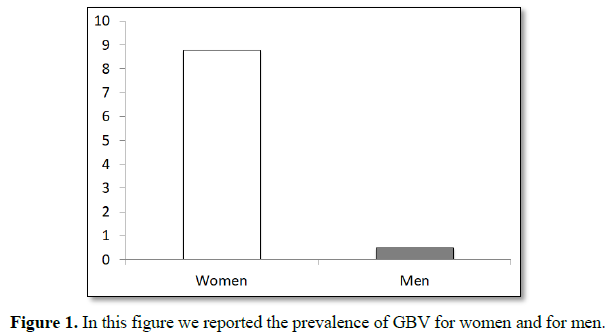
Epidemiologies
The lifetime prevalence of
rape by an intimate partner was an estimated 8.8% for women and an estimated
0.5% for men (Figure 1). An estimated 15.8% of women and 9.5% of men
experienced other forms of sexual violence by an intimate partner during their
lifetimes. Severe physical violence by an intimate partner was experienced by
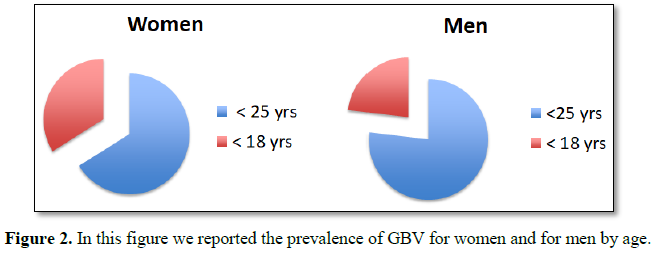
an estimated 22.3% of women and 14.0% of men during their lifetimes. Among
female victims of completed rape, an estimated 78.7% were first raped before
age 25 years, with 40.4% experiencing rape before age 18 years. Among male
victims who were made to penetrate a perpetrator, an estimated 71.0% were
victimized before age 25 years and an estimated 21.3% were victimized before
age 18 years (Figure 2) [4].
In one cross sectional
study, 11.7% of women visiting a variety of American emergency departments were
there because of acute injury or stress related to domestic violence. The
lifetime prevalence rate for domestic violence of 54.2% in women attending Emergency
Departments (ED) [5]
In a study population 12.6%
of men attending emergency departments were victims of domestic violence by a
current or former female intimate partner [6]. These data demonstrate how
important GBV is to an emergency physician.
Risk factors
Individual factors:
·
Young age
·
Heavy drinking
·
Depression
·
Personality disorders
·
Low academic achievement
·
Low income
·
Witnessing or experiencing violence as a child
Relationship factors:
·
Marital conflict
·
Marital instability
·
Male dominance in the family
·
Economic stress
·
Poor family functioning
Community factors:
·
Weak community sanctions against domestic violence
·
Poverty
·
Low social capital
Social factors:
·
Traditional gender norms
·
Social norms supportive of violence [7-10]
Health consequences
GBV has both physical and
psychological consequences.
Physical:
· Headaches
·
Back pain and other musculoskeletal pain
·
Chest pain
·
Gynecological disorders including menstrual disorders, pelvic pain and
dyspareunia
·
Sexually transmitted diseases, including HIV/AIDS
·
Gastrointestinal disorders
·
Urinary tract infection
·
Acute respiratory infection
Psychological:
·
Anxiety
·
Substance use
·
Tobacco use
·
Family and social problems
·
Depression [11]
MANAGEMENT IN ED
An American study identified that
emergency department use was common in the two years before murder by a
partner. In USA, a spouse or intimate partner perpetrated 33.6% of female
homicides, while less than 8% of murders of men were perpetrated by a spouse or
intimate partner [5].
a. How to detect GBV?
It seems that history taking and
clinical examination is unsatisfactory for diagnosing domestic violence. While
the evidence does not support screening for domestic violence, it is still
important that emergency physicians know how to create the opportunity of a
patient disclosing domestic violence, so that self-reported victims of domestic
violence can be offered help. Ideally all consultations should take place in a
private room with, initially, only the patient and the doctor. Simple, direct,
non-judgmental questions are the best way to inquire about domestic violence if
this is felt appropriate. The partner violence scale (PVS) consists of three
questions (Have you been hit, kicked, punched or otherwise hurt by someone
within the past year? Do you feel safe in your current relationship now? Is
there a partner from a previous relationship who is making you feel unsafe
now?) That have been compared with both the index spouse abuse (ISA) and the
conflict tactics scale (CTS), two validated measures of domestic violence. The
first question proved to be nearly as useful as all three questions at
identifying victims. The sensitivity of the PVS compared with the ISA was 65%;
specificity was 80% with a positive predictive value of 51% [5].
b. Management of an identified victim
As always the priority is to
treat the physical injury. It should be explained to the victim that domestic
violence is unacceptable and against the law. Police contact should be offered
while in the comparative safety of the emergency department. It is much easier
to contact the police from the emergency department than a household that is
shared with the perpetrator [5].
SPECIAL CASES
Elder abuse
The definition developed by
Action on Elder Abuse in the United Kingdom and adopted by the International
Network for the Prevention of Elder Abuse states that: “Elder abuse is a single
or repeated act or lack of appropriate action, occurring within any
relationship where there is an expectation of trust which causes harm or
distress to an older person.” Such abuse is generally divided into the
following categories:
·
Physical abuse – the infliction of pain or injury,
physical coercion or physical or drug induced restraint.
·
Psychological or emotional abuse – the infliction of
mental anguish.
·
Financial or material abuse – the illegal or improper
exploitation or use of funds or resources of the older person.
·
Sexual abuse – non-consensual sexual contact of any kind
with the older person.
·
Neglect – the refusal or failure to fulfil a caregiving
obligation. This may or may not involve a conscious and intentional attempt to
inflict physical or emotional distress on the older person.
The rate of abuse is 4-6% among
older people if physical, psychological and financial abuse and neglect are all
included. For older people, the consequences of abuse can be especially
serious. Older people are physically weaker and more vulnerable than younger
adults, their bones are more brittle and convalescence takes longer. Even a
relatively minor injury can cause serious and permanent damage. Many older
people survive on limited incomes, so that the loss of even a small sum of
money can have a significant impact. They may be isolated, lonely or troubled
by illness, in which case they are more vulnerable as targets for fraudulent
schemes.
The medical profession has played
a leading role in raising public concern about elder abuse. While it may be
thought that doctors are best placed to notice cases of abuse – partly because
of the trust that most elderly people have in them – many doctors do not
diagnose abuse because it is not part of their formal or professional training
and hence does not feature in their list of differential diagnoses. Most
emergency departments do not use protocols to detect and deal with elder abuse,
and rarely attempt to address the mental health or behavioral signs of elder
abuse, such as depression, attempted suicide, or drug or alcohol abuse [7].
There should be an
investigation of a patient’s condition for possible abuse if a doctor or other
health care worker notices any of the following signs:
·
Delays between injuries or illness and seeking medical attention;
·
Implausible or vague explanations for injuries or ill-health, from either
the patient or his or her caregiver;
·
Differing case histories from the patient and the caregiver;
·
Frequent visits to emergency departments because a chronic condition has
worsened, despite a care plan and resources to deal with this in the home;
·
Functionally impaired older patients who arrive without their main
caregivers;
·
Laboratory findings that are inconsistent with the history provided.
When conducting an
examination the doctor or health care worker should:
·
Interview the patient alone, asking directly about possible physical
violence, restraints or neglect;
·
Interview the suspected abuser alone;
·
Pay close attention to the relationship between and the behavior of, the
patient and his or her suspected abuser;
·
conduct a comprehensive geriatric assessment of the patient, including
medical, functional, cognitive and social factors;
·
Document the patient’s social networks, both formal and informal [12].
Child abuse
The WHO Consultation
on Child Abuse Prevention drafted the following definition [8]: “Child abuse or
maltreatment constitutes all forms of physical and/or emotional ill-treatment,
sexual abuse neglect or negligent treatment or commercial or other
exploitation, resulting in actual or potential harm to the child’s health,
survival, development or dignity in the context of a relationship of
responsibility, trust or power” [13].
There are four types
of child maltreatment by caregivers, namely:
·
Physical abuse;
·
Sexual abuse;
·
Emotional abuse;
·
Neglect
According to the
World Health Organization, there were an estimated 57 000 deaths attributed to
homicide among children under 15 years of age in 2000. Global estimates of
child homicide suggest that infants and very young children are at greatest
risk, with rates for the 0-4 year old age group more than double those of 5-14
year olds. World for children under 5 years of age living in high-income
countries, the rate of homicide is 2.2 per 100 000 for boys and 1.8 per 100 000
for girls. In low- to middle-income countries the rates are 2-3 times higher –
6.1 per 100 000 for boys and 5.1 per 100 000 for girls [7]. Ill health caused
by child abuse forms a significant portion of the global burden of disease.
Importantly, there is now evidence that major adult forms of illness –
including ischemic heart disease, cancer, chronic lung disease, irritable bowel
syndrome and fibromyalgia – are related to experiences of abuse during
childhood. The apparent mechanism to explain these results is the adoption of
behavioral risk factors such as smoking, alcohol abuse, poor diet and lack of
exercise. Research has also highlighted important direct acute and long-term
consequences [14,15].
Other survivors have
serious psychiatric symptoms, such as depression, anxiety, substance abuse,
aggression, shame or cognitive impairments. Finally, some children meet the
full criteria for psychiatric illnesses that include post-traumatic stress
disorder, major depression, anxiety disorders and sleep disorders [16]. Studies
in various countries have highlighted the need for the continuing education of
health care professionals on the detection and reporting of early signs and
symptoms of child abuse and neglect [17]. In the United States the American
Medical Association and the American Academy of Pediatrics have produced
diagnostic and treatment guidelines for child maltreatment and sexual abuse
[18].
Domestic violence among male patients
In a study population 12.6% of men attending emergency departments were victims of domestic violence by a current or former female intimate partner. In 1978, Steinmetz described “the battered husband syndrome.” She suggested that violence committed by women against their male partners had been largely ignored for several reasons. First, there is a stigma associated with being a man beaten by a woman. Therefore, men are unlikely to admit that they have been assaulted by their partners. Second, injuries inflicted by women on men tend to be less severe and presumably less visible. Finally, there has been little research or media attention on the subject. The most common types of abuse involved unarmed physical assaults and throwing of objects. The use of weapons was less common. Few victims sought help of any type, whether it is legal action, medical attention or counseling [6].
ITALIAN LEGISLATION ABOUT GBV
The first significant
legislative innovation in the field of sexual violence, in Italy, took place
with the approval of the Law of 15 February 1996, n. 66, which began to
consider violence against women as a crime against personal freedom, innovating
the previous legislation, which placed it among the crimes against public
morality and good morals.
With the Law 4 April
2001, n. 154 new measures are introduced aimed at combating cases of violence
within the home with the removal of the violent family member. In the same year
the Laws n. 60 and the Law of 29 March 2001, n. 134 on legal aid for women,
without financial means, raped and/or ill-treated, a fundamental instrument to
defend them and assert their rights, in collaboration with the anti-violence
centers and the courts.
With the Law of 23
April 2009, n. 38 penalties for sexual violence have been exacerbated and the
crime of persecutory acts or stalking is introduced.
Italy has taken a
historic step in the fight against gender violence with the law of 27 June 2013
n. 77, approving the ratification of the Istanbul Convention, drawn up on May
11, 2011. The guidelines outlined by the Convention are in fact the track and
the lighthouse to implement effective measures, at national level, and to
prevent and combat this phenomenon. On October 15, 2013 Law 119/2013 was
approved (in force since October 16, 2013) “Conversion into law, with
amendments, of the decree-law 14 August 2013, n. 93, which contains urgent
provisions on security and to combat gender-based violence”. On 24 November
2017, “the National Guidelines for Aziende Sanitarie and Aziende Ospedaliere on
the issue of relief and social-health assistance to women victims of violence”
were approved.
CONCLUSION
The aim of the
guidelines is to provide an adequate and integrated intervention in the
treatment of the physical and psychological consequences that male violence
produces on women's health. The provision provides, after the nursing triage,
unless it is necessary to assign an emergency code (red or equivalent), that
the woman is recognized a codification of relative urgency (yellow code or
equivalent) to ensure a timely medical examination (time of maximum waiting
time 20 min) and minimize the risk of voluntary repentance or departure.
The guidelines also
provide for the continuous updating of operators and operators, essential for a
good reception, taking charge, risk detection and prevention [19].
1. Policy
and Programme Guidance: HIV and gender-based violence. UN Women Regional Office
for Asia and the Pacific. WHO.
2. Khan
A (2011) Gender-based violence and HIV: A program guide for integrating
gender-based violence prevention and response in PEPFAR programs. Arlington,
VA: USAID’s AIDS Support and Technical Assistance Resources, AIDSTAR-One, Task
Order 1.
3. Ellsberg
M, Heise L (2005) Researching violence against women: A practical guide for
researchers and activists. Washington DC, United States: World Health
Organization, PATH.
4. Breding
MJ (2014) Prevalence and characteristics of sexual violence, stalking and
intimate partner violence victimization — National Intimate Partner and Sexual
Violence Survey, United States, 2011. MMWR Surveill Summ 63: 1-18.
5. Boyle
A, Robinson S, Atkinson P (2004) Domestic violence in emergency medicine
patients. Emerg Med J 21: 9-13.
6. Mechem
CC, Shofer FS, Reinhard SS (1999) History of domestic violence among male
patients presenting to an urban emergency department. Acad Emerg Med 6.
7. Krug
E, Dahlberg LL, Mercy JA (2002) World report on violence and health. Geneva,
World Health Organization.
8. McCloskey
LA, Lichter E, Ganz ML (2005) Intimate partner violence and patient screening
across medical specialties. Acad Emerg Med 12: 712.
9. Crandall
ML, Nathens AB, Kernic MA (2004) Predicting future injury among women in
abusive relationships. J Trauma 56: 906.
10. Khalifeh
H, Oram S, Trevillion K (2015) Recent intimate partner violence among people
with chronic mental illness: Findings from a national cross-sectional survey.
Br J Psychiatry 207: 207.
11. Bonomi
AE, Anderson ML, Reid RJ (2009) Medical and psychosocial diagnoses in women
with a history of intimate partner violence. Arch Intern Med 169: 1692-1697.
12. Lachs
MS, Pillemer KA (1995) Abuse and neglect of elderly persons. N Engl J Med 332:
437-443.
13. WHO
(1999) Report of the Consultation on Child Abuse Prevention. Geneva, World
Health Organization.
14. Anda
R (1999) Adverse childhood experiences and smoking during adolescence and
adulthood. J Am Med Assoc 282: 1652-1658.
15. Felitti
V (1998) Relationship of childhood abuse and household dysfunction to many of
the leading causes of death in adults. Am J Prev Med 14: 245-258.
16. Fergusson
DM, Horwood MT, Lynskey LJ (1996) Childhood sexual abuse and psychiatric
disorder in young adulthood. II: Psychiatric outcomes of childhood sexual
abuse. Journal of the American Academy of Child and Adolescent Psychiatry 35:
1365-1374.
17. Alpert
EJ (1998) Family violence curricula in US medical schools. Am J Prev Med 14:
273-278.
18. American
Academy of Pediatrics (1999) Guidelines for the evaluation of sexual abuse of
children: Subject review. Pediatrics 103: 186-191.